This project has been rather tricky for me to handle; the facts do not add up to what I see as a solid logical solution to wait times and what I would call an “overburdened” hospital system. On the one hand, there is a severe issue in healthcare operations in Canada. Ontario decided that semi-privatization (if you can call it that) was the way to shift some of the burdens outside of the public domain. On paper, it sounds great, but the policy is a massive warning sign of the mishandling of Ontario’s public health system.
The three most important factors I found in all my research are:
- There is not a large-scale funding crisis in Canadian healthcare systems. Per-capita spending has risen dramatically since the Covid-19 pandemic, and it still has not helped solve many issues in Canada’s healthcare system (OECD). This would point to allocation issues instead of direct value of funding issues.
- There was already data that suggested that off-loading some of the less critical or less essential surgeries and diagnostics does not make a discernible impact (BC and Saskatchewan), and specifically in the case of Saskatchewan, backfired.
- An easy solution was for the government to talk with healthcare providers to try and determine the most efficient way of improving wait times and the overall “health” of the healthcare system.
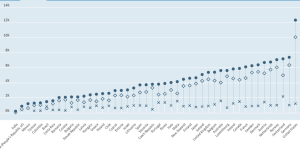
http://data.oecd.org/healthres/health-spending.htm ( Spending per-capita years 2018-2021)
These three factors bothered me immensely because they showed a lack of understanding of the fundamental issues in the “healthcare crisis,” and the solution was neither well-thought-out nor adequately researched. It also shocked me that these were duplicate services insofar as the public sector already covers every operation or diagnostic service that the private clinics would offer.
As a way of sharing my thoughts more structurally, I wanted to think through this problem logically and show my logic pattern in steps:
- There is a problem in the healthcare system with staffing shortages, mainly through the exodus of many nurses and doctors leaving for “greener pastures” or being overstressed and overworked. Covid 19 was the fire, but it was not the instigator.
- Surgeries cannot be managed as wait times balloon because of staffing shortages and hold-ups in Ontario hospitals.
- One of the solutions is to ensure that hospitals can free up wait times by having the proper staffing and equipment needed to perform the operations and diagnostics.
- Moving people to separate clinics opens up more “free” time allocating to hospital operating and Emergency rooms.
- Since the public sector already has these facilities, and they are at capacity, we must look to the private sector to shore up our inefficiencies in Ontario hospitals.
- Private clinics will be equally or better equipped than hospitals if for-profit and incentivized to compete for demand.
The major problem and the one that is causing the most issue is section two from the above list. In particular, the most crucial factor missing from this is the human element. Where will these private clinics find the nurses, staff, and surgeons to run what the hospitals cannot? The private sector is likely more attractive and lucrative than any public hospital. Is this good for the nurses and doctors? One could argue it is good since the wages and stress levels are more manageable. Nevertheless, is it suitable for the public as a whole? No, quite the opposite.
Instead of looking at the long-term implications of the policy, the Ontario government has opted for a short-term gain. It does not make sense in any form or capacity. It reeks of a policy thought without input from an expert, following a flawed system. The solutions were sitting right in front of the policymakers — all they had to do was ask what help the hospitals and primary physicians needed to beef up Ontario’s healthcare.
________________________________________________________________
References