The big question is whether allowing private healthcare clinics to perform surgeries covered under OHIP efficiently uses healthcare policy and funding. As mentioned in a previous editorial blog post, I wrote that there is the ever-present question of where the money given by the government ends up when in public hands. There may even be the case that we are overspending on healthcare, just not in the right areas. This funding problem is the most likely conclusion, as funding has been the highest ever since the inception of the Canada Health Act. There is also the fact that within the OECD, Canada’s healthcare system is in a unique spot where it lacks “comprehensiveness because it covers unlimited demand to a narrow range of services” such as physicians and hospitals (Lee et al., 2021).
Recently, the funding increase proposed by the Federal government will see massive budget spending implications for the Canada Health Transfer (CHT) (Canada Health, 2023). Despite the controversy surrounding the healthcare talks between the federal and provincial governments, which saw the federal government demand funding constraints, healthcare funding is on an ever-upward trajectory (Scherer, 2022). So why the need for private health clinics? The most likely reason is that the Ford government is trying to inject American-style healthcare that benefits for-profit clinics instead of the public sector. Another likely reason is that the provincial government wants to try and reduce wait times as fast as possible, and it does not consider future cost and important step. On the surface, it seems like an abysmal political choice to push privatized healthcare in a country that prides itself on its public healthcare infrastructure. To some, it might be considered prudent to try and fix the problem as quickly as possible, but at what cost to Ontarians?
It seems inevitable that costs would be higher than they would have otherwise been when the government comes to pay the bill for private procedures. CBC News recently looked at who won when provinces contract health care and found that not only were private, for-profit clinics charging more on average, the provincial government would not even give an estimate for the potential cost to taxpayers (CBC News, 2023).

CBC News: https://www.youtube.com/watch?v=GSZW5bw7kXA
Looking at other provinces, Ontario also has excellent examples, such as British Columbia (BC) and Saskatchewan, which have the same type of private-public policies. BC has had policies that allow it to contract certain low-risk elective surgeries, such as cataract surgery and hip and knee placement, for two decades (Longhurst, 2022). It has not shown the increase of the BC provincial government but has also exacerbated queue-jumping issues and overspending due to upcharges by private practitioners (Longhurst, 2022). Saskatchewan has also attempted a “Pilot project” that offered privately provided MRIs for those willing to pay. It did not work. Wait times miraculously increased!
Pictured below are the graphs of percentile wait time taken for minor surgeries such as cataracts or knee and hip replacement by the Canadian Institute for Health Information (CIHI) – the higher the number, the better. Ontario has an even better track record for wait times than BC despite private contracts in place. It is clear that Ontario already has a robust system in place to accelerate wait times for non-essential surgeries. Overall, it seems that the proposed plan to open up private clinics was not fully implemented or thought using the available data.

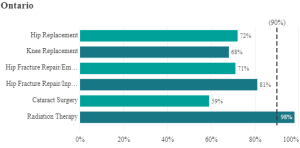
https://www.cihi.ca/en/explore-wait-times-for-priority-procedures-across-canada
The proposed plans outlined by the Ontario provincial government are a good case study of acting in the short term without considering the long-term costs. Of course, it makes sense that the government would want to reduce hospital wait time. It is also logical to assume that opening up the possibility of a closer partnership with private clinics to perform surgeries and diagnostics should shorten the wait times. In the end, the proof is that it does not work. Both BC and Saskatchewan have tried this type of policy, and it has not worked out in the way that the Ontario Government is hoping it will; wait times might decrease in the short term, but when it comes time to pay the bills or look closely at the long term implications of wait times, it does not add up. The Ontario provincial government has the right goal but it is just the wrong solution.
___________________________________________________________________________________________
References
Agecoutay, C., & Jones, A. M. (2022, August 21). ‘I thought I might die at home’: Canada’s healthcare system is crumbling, experts say. CTVNews. https://www.ctvnews.ca/health/i-thought-i-might-die-at-home-canada-s-health-care-system-is-crumbling-experts-say-1.6036628
Canada, H. (2023, February 7). Working together to improve health care for Canadians. https://www.canada.ca/en/health-canada/news/2023/02/working-together-to-improve-health-care-for-canadians.html
CBC News (2023, March 6). Who wins when provinces contract health care? | About That. https://www.youtube.com/watch?v=GSZW5bw7kXA
Lee SK, Rowe BH, Mahl SK. Increased Private Healthcare for Canada: Is That the Right Solution? Healthcare Policy. 2021 Feb;16(3):30-42. doi: 10.12927/hcpol.2021.26435. PMID: 33720822; PMCID: PMC7957357.
Longhurst, A. (2022, August 26). The concerning rise of corporate medicine: Public contracts with private clinics top $393 million over last six years. Policy Note. https://www.policynote.ca/corporate-medicine/
Scherer, S. (2022, December 22). Canada’s politicians fight over spending on strained healthcare system. Reuters. https://www.reuters.com/world/americas/canadas-politicians-fight-over-spending-strained-healthcare-system-2022-12-22/